Bedsores (decubitus - decubitus ulcer) are chronic soft tissue ulcers that occur in patients with impaired sensitivity (usually immobile) due to compression, friction or displacement of the skin, or as a result of a combination of these factors.
ICD-10 code
L89. Bedsores
ICD-10 code
Epidemiology
The incidence of pressure ulcers in hospitalized patients ranges from 2.7 to 29%, reaching 40-60% in patients who have suffered a spinal cord injury. In health care settings in England, pressure ulcers develop in 15-20% of patients. The organization of high-quality care provided by specially trained caregivers can reduce the incidence of this complication to 8%.
Treatment of patients with pressure ulcers is a serious medical and social problem. With the development of pressure ulcers, the duration of the patient’s hospitalization increases, and there is a need for additional dressings and medicines ah, tools, equipment. In some cases, surgical treatment of bedsores is required. The estimated cost of treating pressure ulcers per patient in the United States ranges from $5,000 to $40,000. In the UK, the cost of caring for patients with pressure ulcers is estimated at £200 million, rising by 11% annually.
In addition to the economic costs associated with the treatment of bedsores, it is necessary to take into account intangible costs: severe physical and mental suffering experienced by the patient. The occurrence of bedsores is often accompanied by severe pain, depression, and infectious complications (abscess, purulent arthritis, osteomyelitis, sepsis). The development of pressure ulcers is accompanied by an invariably high mortality rate. Thus, the mortality rate in patients admitted to nursing homes with bedsores, according to various sources, ranges from 21 to 88%.
Why do bedsores occur?
Most often, bedsores are found in long-term immobilized patients who are in a forced position after an injury, with oncological and neurological pathologies, in elderly and senile people with severe therapeutic diseases, as well as in patients undergoing long-term treatment in intensive care units.
The main factors leading to the development of bedsores are forces of pressure, displacement and friction, and increased humidity. Risk factors include limited physical activity of the patient, malnutrition or obesity, urinary and fecal incontinence, defects in care, concomitant diseases such as diabetes, paralysis and cancer. A significant risk factor is being male and the age of the patient. In patients over 70 years of age, the risk of pressure ulcers increases sharply. Among the social factors, the lack of service personnel should be noted.
Ulcers resulting from pressure ulcers are areas of tissue necrosis that occur in weakened individuals as a result of compression by one’s own body of the soft tissues directly adjacent to the bones and bony protrusions. Prolonged exposure to continuous pressure leads to local tissue ischemia. It has been experimentally and clinically established that pressure of 70 mmHg, exerted on tissue continuously for two or more hours, leads to irreversible changes in tissue. However, with periodic pressure of even greater force, tissue damage is minimal.
The combined effect of pressure and displacement forces causes disturbances in blood flow with the development of irreversible tissue ischemia and subsequent necrosis. Muscle tissue is most sensitive to ischemia. In the muscles located above the bony protrusions, pathological changes first develop, and only then do they spread towards the skin. The addition of infection aggravates the severity of ischemic tissue damage and contributes to the rapid progression of the necrosis zone. The resulting skin ulcer in most cases is a kind of tip of the iceberg, while 70% of all necrosis is located under the skin.
Risk factors for developing pressure ulcers
One of the main stages of pressure ulcer prevention is to identify patients at high risk. Risk factors for the development of pressure ulcers can be reversible and irreversible, internal and external. Internal reversible risk factors are exhaustion, limited mobility, anemia, low nutrition, insufficient intake of ascorbic acid, dehydration, hypotension, urinary and fecal incontinence, neurological disorders, impaired peripheral circulation, thin skin, anxiety, confusion and coma. External reversible risk factors include poor hygienic care, folds in bedding and underwear, bed rails, use of patient restraints, injuries to the spine, pelvic bones, abdominal organs, spinal cord injuries, use of cytostatic drugs and glucocorticoid hormones, improper moving technique patient in bed. External risk factors for the development of bedsores include extensive surgical intervention lasting more than 2 hours.
Various scales provide significant assistance in assessing the degree of risk of developing pressure ulcers. The most widely used scale is J. Waterlow. In immobile patients, the risk of developing pressure ulcers is assessed daily, even if during the initial examination it was no more than 9 points. Anti-bedsore measures begin immediately when there is a high risk of their development.
Scores on the J. Waterlow scale are summed up. The degree of risk is determined by the following total values:
- no risk - 1-9 points;
- there is a risk - 10-14 points;
- high risk - 15-19 points;
- very high risk level - more than 20 points.
Symptoms of bedsores
The location of pressure ulcers can be extremely varied. The frequency of identifying the location of pressure ulcers depends on the specialization of the clinic or department. In multidisciplinary hospitals, the vast majority of patients develop bedsores in the sacral area. Quite often the area of the greater trochanter, heels and ischial tuberosities is affected. In more rare cases, a decubital ulcer occurs in the area of the shoulder blades and lateral surfaces chest, bony protrusions of the spine, extensor surfaces knee joints and on the back of the head. Multiple bedsores occur in 20-25% of cases.
At the beginning of the development of a bedsore, local pallor, cyanosis and swelling of the skin appear. Patients complain of a feeling of numbness and slight soreness. Later, detachment of the epidermis occurs with the formation of blisters filled with turbid serous-hemorrhagic exudate, necrosis of the skin and underlying tissues occurs. Infection aggravates the severity of necrotic tissue damage.
Clinically, bedsores occur as dry or wet necrosis (decubital gangrene). When a pressure sore develops according to the type of dry necrosis, the wound looks like a dense necrotic scab with a more or less distinct line of demarcation of non-viable tissue. Due to mild pain and mild intoxication, the patient’s general condition does not suffer significantly. A more severe clinical picture is observed with the development of a pressure sore of the wet necrosis type. The zone of deep irreversible tissue ischemia does not have a clear boundary and rapidly progresses, spreading not only to the subcutaneous tissue, but also to the fascia, muscles, and bone structures. The surrounding tissues are edematous, hyperemic or cyanotic, and sharply painful on palpation. From under the necrosis, foul-smelling purulent discharge flows abundantly gray. Symptoms of severe intoxication are noted with a rise in body temperature to 38-39 ° C and above, accompanied by chills, tachycardia, shortness of breath and hypotension. The patient becomes drowsy, apathetic, refuses to eat, and becomes delirious. Blood tests reveal leukocytosis, increased ESR, progressive hypoproteinemia and anemia.
Classification
There are several classifications of pressure ulcers, but currently the most widespread is the classification adopted in 1992 by the Agency for Health Care Policy and Research (USA), which most clearly reflects the dynamics of local changes in the field of pressure ulcers:
- I degree - erythema that does not extend to healthy areas of the skin; damage preceding ulceration;
- II degree - partial reduction in skin thickness associated with damage to the epidermis or dermis; a superficial ulcer in the form of an abrasion, blister, or shallow crater;
- III degree - complete loss of skin thickness due to damage or necrosis of tissue located underneath it, but not deeper than the fascia;
- IV degree - complete loss of skin thickness with necrosis or destruction of muscles, bones and other supporting structures (tendons, ligaments, joint capsules).
Classification of bedsores by size:
- fistula form - a small skin defect with a significant deeper cavity; often accompanied by osteomyelitis of the underlying bone;
- small bedsore - diameter less than 5 cm;
- average bedsore - diameter from 5 to 10 cm;
- large bedsore - diameter from 10 to 15 cm;
- giant bedsore - diameter more than 15 cm.
According to the mechanism of occurrence, bedsores are distinguished as exogenous, endogenous and mixed. Exogenous bedsores develop as a result of prolonged and intense exposure to external mechanical factors leading to ischemia and tissue necrosis (for example, a bedsore as a result of tissue compression by a plaster cast or a bedsore of the sacrum in a patient who has been in a stationary position for a long time). Eliminating the causes of a bedsore usually promotes the development of reparative processes and its healing. Endogenous pressure ulcers develop due to disruption of the body’s vital functions, accompanied by neurotrophic changes in tissue as a result of diseases and damage to the central and peripheral nervous system(for example, in patients with spinal injury and stroke). Healing of such bedsores is possible with improvement of the general condition of the body and tissue trophism. Mixed bedsores develop in patients weakened and exhausted by a serious illness, nutritional cachexia. The inability to independently change body position as a result of prolonged tissue compression leads to ischemic skin damage in the area of bone protrusions and the formation of bedsores.
There are also external and internal bedsores. External pressure ulcers develop in the area skin. Internal pressure ulcers occur in various areas of the mucous membranes that are subject to prolonged compression by foreign bodies (drains, catheters, prostheses and stents) and endogenous formations (calculus). gallbladder). Internal bedsores can lead to perforation of the organ wall with the development of an internal fistula, peritonitis, phlegmon and other complications.
Complications of bedsores aggravate the condition of patients, worsen the prognosis of the disease, most of them representing real threat for the life of the patient, becoming one of the main causes of death of patients. These include:
- contact osteomyelitis of the underlying bone;
- purulent arthritis and tendinitis;
- erosive bleeding;
- malignancy;
- phlegmon;
- sepsis.
Osteomyelitis occurs in almost 20% of patients with pressure ulcers. Most often the sacrum, coccyx bones, ischial tuberosity, calcaneus, and occipital bones are affected. The most severe osteoarticular destructive changes occur in patients with pressure sores in the greater trochanter area. Osteomyelitis of the greater trochanter develops, and in more severe cases - purulent coxitis, osteomyelitis of the head of the femur and pelvic bones. The diagnosis is made on the basis of a visual assessment of the bone, which takes on a dull appearance, has a gray color, lacks periosteum, is saturated with purulent exudate, becomes brittle on contact, and bleeds little. If there are difficulties in diagnosis, X-ray examination, fistulography, CT and MRI are used. It should be noted that clear radiological data appear in the late stages of development of osteomyelitis with extensive bone lesions and sequestration.
Cellulitis is the most severe complication of bedsores. It develops in 10% of patients with pressure ulcers and is the main reason for emergency hospitalization of patients. Cellulitis mainly complicates the course of bedsores that occur as wet necrosis. At the same time, a significant deterioration in the patients’ condition is noted, symptoms of a systemic inflammatory reaction progress, pain syndrome, signs of organ dysfunction develop. Local changes have negative dynamics. Perifocal inflammatory changes increase significantly. Hyperemia, edema and tissue infiltration spread over a large area; Cyanotic spots and blisters appear both on the skin around the bedsore and at a distance from it. With a large accumulation of pus, fluctuation can be determined, and with the anaerobic nature of the infection, tissue crepitus appears. Cellulitis usually develops as a result of a delay in surgical debridement during the development of wet decubital gangrene. The purulent-necrotic process begins in the deep layers of soft tissue, quickly progresses and is accompanied by severe destructive changes in the tissues with the development of necrotizing dermatocellulitis, fasciitis and myonecrosis. In more than 80% of all cases of phlegmon, it occurs in patients with bedsores of the sacrum. The purulent process can spread to the gluteal and lumbar regions, perineum, back of the thigh. In the vast majority of cases, the purulent-necrotic process is caused by polyvalent microflora. The main role is played by microbial associations consisting of Staphylococcus aureus, Streptococcus spp., Enterococcus spp., bacteria from the genus Enterobacteriaceae, Pseudomonas aeruginosa, anaerobic clostridial and non-clostridial infections. In exhausted, weakened elderly and senile patients, the mortality rate when phlegmon occurs against the background of a bedsore exceeds 70%.
Three main factors lead to the formation of bedsores:
First factor the one most often mentioned is pressure. Due to body pressure, tissue (skin, muscles) is compressed between the surface on which it rests and the protrusions of the bones. This compression of vulnerable tissues is further intensified by heavy bedding, tight bandages, or a person's clothing, including shoes in patients who are sitting still.
Second factor, which is practically not mentioned, "shear". Destruction and mechanical damage to tissue occurs under the influence of indirect pressure. It is caused by a shift of tissues relative to the surface, or their “cutting”. Shift of tissues is observed if a person slides down from the pillows in bed, or pulls himself up towards the head of the bed, as well as when staff or relatives use the wrong technique to move the patient. This factor can cause tissue damage as deep as direct pressure. In more serious cases, muscle fibers and lymphatic vessels even rupture, leading to the formation of deep bedsores. Moreover, deep damage can become noticeable only after some time, since the skin located above it can remain intact for two weeks.
Third factor, which is also practically not mentioned, - friction as a component of "shear force". It causes peeling of the stratum corneum of the skin, leading to ulceration of its surface. Friction increases as the skin becomes hydrated. People are most susceptible to it when they are urinary incontinent, sweating, wearing damp and non-absorbent (synthetic) underwear or sitting on non-absorbent surfaces (plastic chairs, oilcloths or bedding that is not regularly changed).
Under normal conditions, none of these factors leads to the formation of bedsores, but in combination with others - immobility, loss of sensitivity, anemia, depression, etc., they pose a risk.
There are other reasons that predispose to the development of pressure sores:
- too much or too little body weight;
- dry skin and resulting cracks;
- urinary and/or fecal incontinence and excessive wetness;
- vascular diseases leading to disruption of tissue nutrition;
- anemia;
- limitation of the patient's mobility due to:
- the patient’s admission to the hospital and the lack of mobility assistance to which he is accustomed at home;
- use of sedatives and analgesics;
- apathy and depression;
- damage to the motor centers of the brain and spinal cord;
- pain;
- increase or decrease in body temperature;
- insufficient protein nutrition.
Thus, the most susceptible to the effects of the above factors are: the elderly; patients with spinal cord injury; receiving sedatives and analgesics; with limb damage; in a state of cachexia; with low resistance to infection; not receiving enough protein foods.
Secondary factors leading to the development of bedsores: urinary and/or fecal incontinence; wet underwear; incorrect technique for moving the patient; hard surfaces on which the patient sits (lies); prolonged sitting in bed (on a chair); incorrect body position; inability (ignorance) to use devices that relieve pressure.
It is the secondary factors that should be primarily in the field of view of nursing staff. To do this, the nurse must, firstly, clearly understand the potential danger of these factors on the patient, and secondly, know the principles of preventing bedsores and their capabilities, as well as a preliminary assessment system that allows them to identify patients at risk.
The topic of the article is the classification of bedsores, how to recognize the different stages of bedsores in time, what types and degrees of bedsores exist. This information will help you respond to danger in a timely manner and contact a specialist to properly solve the problem.
It can be difficult for relatives caring for a bedridden or sedentary patient to understand what kind of lesion we are talking about and what measures need to be taken. After all, a bedsore refers to both minor damage to the skin, which can be eliminated with proper care, and deep ulcers on the body that pose a threat to life.
Classification of bedsores
Causes and risk factors for the formation of bedsores
The main reason for the formation of bedsores is a person’s prolonged stay in a stationary position. Limitation of mobility may result various situations: injuries, diseases that limit mobility, severe exhaustion, mental illness, coma, etc. Damage to the skin, and then soft tissue, primarily occurs in “bulging” areas of the body, in which there is a very thin thin layer between the bone tissue and the skin layer of fiber (fat tissue) and muscle.

If the patient lies on his back, bedsores most often form in the area of the sacrum, coccyx, thoracic spine, heels, less often - the back of the head, shoulder blades. In the prone position, the knees, the area of the iliac bones (bulging areas of the pelvic bone), and the bulging surface of the chest are more often affected. In the lateral decubitus position, tissues most often affected are the greater trochanter of the femur and the iliac crest. In sedentary patients, lesions often develop in the area of the closure of the buttocks, tailbone, and heels.

 How does a bedsore occur? In the area that is subject to pressure, blood circulation is impaired, causing cells to begin to suffer from a lack of oxygen and nutrients. Also, due to compression of the lymphatic vessels responsible for removing waste products from cells, waste and poisons begin to accumulate, poisoning the internal environment of the cell.
How does a bedsore occur? In the area that is subject to pressure, blood circulation is impaired, causing cells to begin to suffer from a lack of oxygen and nutrients. Also, due to compression of the lymphatic vessels responsible for removing waste products from cells, waste and poisons begin to accumulate, poisoning the internal environment of the cell.
In addition to pressure, factors such as friction, tissue displacement, and moisture play an important role in the development of damage to the skin and underlying soft tissues - you can read more about this. If the influence of the factors causing this entire cascade of damage does not stop, the cells begin to die - tissue necrosis (death) develops, spreading to the skin, subcutaneous fat and muscles.
The risk of developing pressure ulcers also depends on many other factors. Thus, in the Industry Standard " Patient management protocol. Bedsores", developed by the Ministry of Health of the Russian Federation, it is proposed point system(Waterlow scale) to assess the risk of developing pressure ulcers depending on age, gender, the presence of concomitant diseases in the patient, etc. The table below presents some of these criteria:
|
Criterion |
Indicators |
Risk level for developing bedsores (in points) |
|---|---|---|
|
Age (years) |
||
|
Food (features) |
||
|
Obesity |
||
|
Exhaustion |
||
|
Some diseases and bad habits |
Diabetes mellitus |
|
|
Vascular diseases |
||
|
Anemia (anemia) |
||
|
Stroke, diseases and injuries of the brain and spinal cord, paralysis |
||
|
Incontinence |
Periodic diversion of urine through a catheter |
|
|
Fecal incontinence |
||
|
Fecal and urinary incontinence |
There are also types of bedsores that occur as a result of pressure and friction from a cast (or other fixation material), vascular or urinary catheter. In addition, one of the most important reasons for the development of damage to the skin and soft tissues in sedentary patients is low levels. The microvibration background of the body is created due to contractions of muscle cells, which are recorded not only during physical activity, but even at rest and sleep. This valuable resource is as important to sustaining life as air, water, food and heat. It is necessary for metabolic processes in cells and the directed movement of substances through blood and lymphatic vessels.
A sufficient level of microvibration is also needed for the full functioning of the lymphatic system, on which the condition of the body depends, the ability of the body to get rid of toxins, poisons (formed as a result of the vital activity of cells, the death of microbes, etc.), as well as. Maximum saturation of the body with microvibration energy occurs through physical activity - sports, walking, swimming, etc.
People who, for some reason, are deprived of the ability to move actively, and especially patients confined to a bed or wheelchair, develop a pronounced deficiency of microvibration energy in the body. What disorders that contribute to the development of bedsores does this lead to?
- The functioning of blood vessels suffers, which disrupts the delivery of nutrients and oxygen to tissues (including skin and muscle cells).
- Metabolic processes are disrupted in the cells, poisons and waste begin to actively accumulate, which accelerates cell death. Due to disruption of the lymphatic system and other organs (liver, kidneys) responsible for the processes of removing metabolic products from the body, which is also associated with a deficiency of microvibration, poisons and toxins accumulate. This leads to poisoning of the body, decreased organ function and the creation of a favorable environment for the development of pathogenic bacteria.
- Deterioration of the lymphatic system leads to decreased immunity, which also increases the risk of developing infectious complications.
Thus, a deficiency of microvibration accelerates the process of death of skin and muscle cells in patients, promotes the accumulation of dead cells, toxins and poisons in the body, increases the risk of infection: all this creates conditions for the development and progression of bedsores in bedridden patients.
The situation is aggravated by the fact that muscle cells, deprived of the ability to move, begin to decrease in size (atrophy), muscle mass becomes less and less, which leads to a further decrease in the level of microvibration in the body. In this situation, essential support for the body is - about its role in treatment And prevention of bedsores will be discussed further.
What are the stages of development of bedsores? In domestic and foreign medicine, there are different classifications, which are based on different criteria for assessing bedsores - external manifestations and symptoms, depth of tissue damage, cause of occurrence, presence of complications, etc.
The Protocol for the management of patients with pressure ulcers, a key document that all medical institutions in the Russian Federation are guided by, presents a classification that describes the symptoms of pressure ulcers at each stage. This classification is sometimes called dynamic. This definition implies that the dynamics of the process, that is, the transition from one phase to another, is not at all obligatory and immutable, but depends on many reasons and, above all, on proper care (especially in the initial stages). Also, timely resource support for the patient plays an important role - increasing the level of microvibration in the patient’s body.
According to the Protocol, there are 4 stages of pressure ulcers: below is a table that reflects this classification.
|
Stage of bedsore development |
Signs and symptoms |
|---|---|
|
The earliest stage in which the integrity of the skin is not compromised. What do bedsores look like in the initial stages? Visible on the skin at the point of pressure a focus of redness (hyperemia) that does not disappear after the pressure stops. As oxygen starvation increases, skin color changes. How do bedsores (stage 1) begin to look in the photo at this stage? It becomes noticeable that the area under pressure acquires a bluish tint and becomes swollen. The patient notes an increase in sensitivity in the area where the bedsore develops, which intensifies with pressure. Gradually, sensitivity decreases and numbness occurs, which is associated with pinching of nerve endings. |
|
|
Symptoms of this stage are associated with the death (necrosis) of skin cells and the upper layers of subcutaneous fat. First, the superficial layers of the skin (epidermis), and then the deeper ones (dermis), become thinner, and skin detachment occurs. Sign of second degree bedsores – formation of blisters at the site of pressure, peeling. A focus of inflammation may also be observed in the form of an elevation with a depression in the center (the beginning of the formation of an ulcer) |
|
|
Manifestations of this stage are caused by deep necrosis of the skin and subcutaneous fat with penetration into the muscles. The bedsore at this stage looks like wound or ulcer, there may be a discharge of clear or cloudy (purulent) fluid. |
|
|
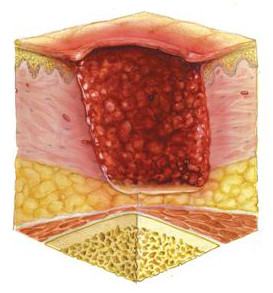
The development of this stage is associated with the death of skin cells, subcutaneous tissue and muscles. Stage 4 bedsores look like a deep wound, at the bottom of which deep-lying tendons, joint elements, and bone tissue can be visible. |
 To better understand what bedsores look like, you can look at the photo: the initial stage is characterized by the presence of a focus of redness, the skin is not damaged, as oxygen deprivation increases, the skin acquires a bluish tint (the development of cyanosis)
To better understand what bedsores look like, you can look at the photo: the initial stage is characterized by the presence of a focus of redness, the skin is not damaged, as oxygen deprivation increases, the skin acquires a bluish tint (the development of cyanosis)
What do bedsores (stage 2) look like in photographs? Here we observe violations of the integrity of the skin - from peeling to the formation of a superficial wound.

In stage 3, the wound becomes deeper and muscle tissue may be visible. What do stage 4 bedsores look like? The photographs show deep wounds, at the bottom of which bones, ligaments, and tendons may be visible.
Classification by stages of the pressure ulcer process
Professor M.D. Dibirov (Department of Surgical Diseases and Clinical Angiology of the A.I. Evdokimov Moscow State Medical University) also talks about the classification of pressure ulcers, focusing on the stage of the pressure ulcer process. In total, there are three stages: in order to understand what bedsores look like in each of them, you can look at the photos by stage.
Stage I – stage of circulatory disorders (vascular disorders)
This stage is characterized by changes caused by impaired blood circulation in the tissues. First, the skin becomes pale at the point of pressure, which is replaced by redness, then the skin acquires a bluish tint. What do bedsores look like in the initial stages? The photo shows areas of redness without clear boundaries, the integrity of the skin is not compromised.
Stage II – stage of necrotic changes and suppuration
At this stage, cell death (necrosis) occurs with damage to the skin and underlying tissues: fiber, muscles. At this stage, an infection may occur that affects both soft tissue (skin, subcutaneous tissue, muscles) and bone and joint tissue.
A bedsore at this stage may look like a superficial wound or a deep ulcer, in some cases having a dry surface and clear edges, in others there is purulent discharge and blurred edges, which indicates the spread of the process to the surrounding tissues.
Stage III – healing stage
At this stage, tissue regeneration (restoration) processes prevail in the area of the pressure sore, the wound heals - the integrity of the skin is restored or a scar is formed.
Classification of bedsores by mechanism of occurrence
Also in medical practice, a classification is used, which is based on the division of pressure ulcers into groups, taking into account the mechanism of their occurrence. In this case, the role of the influence of external causes and internal disorders that play a role in the development of the damage we are talking about is taken into account
There are three types of pressure ulcers: exogenous, endogenous and mixed.
- Exogenous bedsores– damage, the occurrence of which is associated primarily with external influences (from the Greek exo - outside, genes - generated). First of all, we're talking about about damage to the skin and underlying tissues that develop under the influence of factors already mentioned above: pressure (as a key factor), friction, sliding, humidity. In turn, exogenous bedsores are divided into external and internal:
- External exogenous bedsores- these are the same injuries that develop from contact of the most protruding areas of the body (for example, the sacrum, shoulder blades, heels in the “supine” position) with a hard surface. This group also includes injuries resulting from pressure and friction of plaster casts (and other materials used for fixation in case of injuries), various corsets, poorly selected prostheses, etc.
- Internal exogenous bedsores – areas of damaged skin that appear as a result of constant pressure from catheters - tubes inserted into blood vessels to facilitate the administration of drugs, into the urinary canal or bladder for urine drainage. As a rule, they develop in patients with metabolic disorders, exhaustion, and problems with blood supply to tissues.
- Endogenous bedsores(from the Greek endo - inside) are associated primarily with internal disorders in the body. Most often, such injuries occur in patients with lesions of the brain and/or spinal cord. This could be an injury, stroke (hemorrhage), tumor, etc. Such diseases lead to disruption of the nervous regulation of metabolic processes in tissues and disruption of vascular tone. As a result, the nutrition of cells, including muscles and skin, suffers, which is the main reason for the development of damage. Such bedsores are often called neurotrophic ulcers (from the Greek trophe - nutrition).
The main danger of such lesions is that the death of muscle cells and the development of ulcers in muscle tissue often occurs when the skin is intact. Thus, it can be difficult to recognize and take adequate measures to treat them in time - ultrasound examination of soft tissues may be required to diagnose them. That is why patients with diseases and injuries of the nervous system need constant medical supervision.
- Mixed pressure ulcers develop when the body has internal problems (for example, exhaustion, cancer), as a result of which the regulation of tissue nutrition and metabolic processes suffers, and there are external influences - pressure, friction, etc.
 The tactics of their treatment depend on the action of which factors (external or internal) are associated with the formation of bedsores. So, if external reasons play a leading role, then solve the problem (especially early stages) is possible with the help of proper care and well-chosen medications for topical use.
The tactics of their treatment depend on the action of which factors (external or internal) are associated with the formation of bedsores. So, if external reasons play a leading role, then solve the problem (especially early stages) is possible with the help of proper care and well-chosen medications for topical use.
Why is it important to understand what causes damage? Because patient management tactics depend on this. If the problem is primarily related to diseases and injuries of the nervous system, metabolic disorders caused by various diseases, etc., then priority measures should be aimed at improving tissue nutrition, nerve conduction, normalizing metabolism, restoring blood supply to tissues, etc. If external causes play a leading role, then the problem can be solved (especially in the early stages) with the help proper care and well-chosen medications for local use.
At the same time, when we are talking about advanced processes (these are the third and fourth stages), then, for whatever reason, damage occurs, in most cases, surgery is necessary to eliminate it. Besides, All patients suffering from bedsores are recommended vibroacoustic therapy, providing the body with a resource. In this case, the cause of the problem also does not matter.
Classification of bedsores by type of necrosis (cell death)
When, as a result of certain reasons, cells begin to die at the site of the development of a bedsore, an area of necrosis (dead tissue) appears. However, in different cases this process develops differently:
- Dry necrosis(mummification) is the “drying out” of the affected tissues. The lesion has clear boundaries, there is no discharge from the wound: infection occurs very rarely, in the initial stages, when a certain amount of fluid remains in the tissues. The patient may notice pain in the affected area, but the general condition most often does not suffer.
- Wet necrosis(bedsore gangrene) often develops in weakened patients with lesions of the nervous system, metabolic and vascular disorders. In this case, tissue necrosis occurs over large areas, and the damaged area often becomes infected. The wound is swollen, purulent discharge with an unpleasant odor is found in it.
As a rule, the development of pressure ulcer gangrene is accompanied by a sharp deterioration in the patient’s general condition: an increase in temperature, delirium, loss of consciousness, palpitations, and vomiting may be observed (as a consequence of poisoning of the body with microbial decay products). In the absence of adequate measures (prescription of antibiotics, surgical treatment), there is a high probability of developing sepsis - blood poisoning, often leading to the death of the patient.
Classification of pressure ulcers by size (diameter of lesion)
- Small bedsore: diameter less than 5 cm.
- Average bedsore: diameter is 5-10 cm.
- Large bedsore: diameter is up to 10 to 15 cm.
- Giant bedsore: diameter exceeds 15 cm.
It should be noted that a large diameter of a bedsore does not always indicate the presence of a severe process: extensive lesions can sometimes be superficial, occur without infectious complications and respond quite well to treatment without surgery. Of course, this picture is more common when it is not advanced bedsores that are observed, but the initial stage of the process.
 At the same time, an ulcer with a relatively small diameter can be quite deep, reach the muscle layer and serve as an entry gate for infection. A similar picture is often observed in patients with damage to the nervous system and blood vessels.
At the same time, an ulcer with a relatively small diameter can be quite deep, reach the muscle layer and serve as an entry gate for infection. A similar picture is often observed in patients with damage to the nervous system and blood vessels.
In this case, the so-called fistulous form of bedsore - the entrance hole (ulcer) in the area of the skin has a minimal diameter (less than 1 cm), it is a canal that leads into a deep cavity with purulent contents located underneath. Moreover, not only muscles, but also bone tissue can be involved in the inflammatory process with the development of osteomyelitis.
Classification of bedsore complications
Bedsores in patients are often complicated by the addition of an infectious process, especially when it comes to stages 3-4 (the presence of a deep ulcer with damage to muscle tissue). If the patient is in a hospital, there is a high probability of developing inflammation caused by a nosocomial infection, that is, pathogens that are resistant to the action of many antibiotics. When making a diagnosis in the case of complicated pressure ulcers, in addition to the stage of the process, the type of complication is indicated.
Depending on what tissues are involved in the inflammatory process, the following types of infectious complications of bedsores are distinguished:
- Phlegmon– inflammation of subcutaneous fat tissue, connective tissue, which has no clear boundaries. Most often caused by staphylococcus.
- Abscess- a focus of purulent melting of soft tissues (fiber, connective tissue, muscles) with the formation of a purulent cavity, which has clear boundaries.
- Osteomyelitis– melting of bone tissue. More often it occurs in areas such as the coccyx, sacrum, back of the head, and heel bones.
- Suppurative arthritis– inflammation in the joint area.
- Purulent melting of the vascular wall– can lead to both bleeding and the entry of purulent contents into the bloodstream.
- Sepsis– spread of infection throughout the body, and the formation of purulent foci may occur in various organs(heart, kidneys, lungs, joints, etc.) with the development of inflammatory processes in them. The entry into the blood of a large amount of toxic (harmful) substances associated with the massive death and disintegration of cells, living and dead microbes and their metabolic products can very quickly cause the death of the patient.
It is also possible to develop complications such as erysipelas associated with the penetration of streptococci into the pressure wound. In some cases, in the presence of long-term non-healing ulcers, especially in patients with diseases of the nervous system and metabolic disorders, it is possible malignant degeneration (malignancy) and development of skin cancer at the site of a bedsore (Sh.M. Chyngyshpaev, 2013).
 Bedsores do not always develop in patients in the hospital. Often, relatives care for a patient with limited mobility at home. What should you do if you discover the damage that we are talking about in this article?
Bedsores do not always develop in patients in the hospital. Often, relatives care for a patient with limited mobility at home. What should you do if you discover the damage that we are talking about in this article?
First of all, it is necessary to call a doctor who can competently assess the condition of the skin and soft tissues at the site of development of the lesion and, if necessary, make a decision to send the patient to the hospital.
But this is not always necessary. For example, bedsores in which there is no deep tissue damage (as a rule, we are talking about the first and second stages) and there are no signs of an infectious process can be dealt with at home. In this case, the most important role is played by the organization of proper care for the patient, a rational diet and drinking regimen, the formation of a favorable microclimate in the room where the patient is, the use of local medications, etc. You can read more about this in the article “ How to treat bedsores in bedridden patients at home?».
An effective means of treating and preventing bedsores is. Use in people with limited mobility helps to increase levels in the body and solve the following problems:
- Activation of metabolic processes in all organs and tissues, including skin and muscles.
- Improving blood supply to all tissues of the body.
- Stimulation of the process of removal (disposal) of dead cells, toxins and poisons due to improved functioning of the lymphatic system and other organs responsible for cleansing the body (kidneys, liver)
- Strengthening immune system, due to which the risk of developing infectious complications is significantly reduced.
List of used literature:
- Baskov A.V. Surgical treatment bedsores in patients with spinal cord injury / Issues of neurosurgery - 2000 - No. 1
- Vorobiev A.A. Treatment of bedsores in spinal patients / Bulletin of the Volgograd Scientific Center of the Russian Academy of Medical Sciences - 2007 - No. 2
- Garkavi A.V. Complex treatment of bedsores in spinal patients. Dissertation of Candidate of Medical Sciences / Moscow, 1991.
- Dibirov M.D. Bedsores. Prevention and treatment / Medical Council, No. 5-6, 2013.
- Zilovich A. A. Surgical treatment of bedsores, trophic ulcers and osteomyelitis in patients with injuries of the spine and spinal cord. Dissertation of Candidate of Medical Sciences / Donetsk, 1986.
- Klimiashvili A.D. Prevention and treatment of bedsores / Russian Medical Journal – 2004 – T. 12, No. 12.
- Kogan O. G. Classification and combined conservative-surgical treatment of bedsores and bursitis in cases of spinal cord lesions. Methodical recommendations for doctors / Novokuznetsk, 1976
- / “Doctor” No. 7 / 2014
- Musalatov H.A. Treatment of bedsores in patients with injuries of the spine and spinal cord / Medical Care - 2002 - No. 3.
- Patient management protocol. Bedsores /Appendix to the order of the Ministry of Health of Russia dated April 17, 2002. No. 123.
- Fedorov V.A., Kovelenov A.Yu., Loginov G.N. and others / St. Petersburg: SpetsLit, 2012.
You can ask questions (below) on the topic of the article and we will try to answer them competently!
Bedsores are a serious complication in patients with impaired tissue nutrition, both under the influence of external compression and as a result of various systemic diseases.
Bedsore - necrosis (necrosis) of soft tissues due to constant pressure, accompanied by local circulatory and nervous trophism disorders.
Clinically, it is more correct to designate this pathological process as an ulcer formed due to pressure.
Types of bedsores
Grade I: the skin is not damaged. Sustained hyperemia that does not go away after the pressure stops.
Degree II: superficial (shallow) violation of the integrity of the skin extending to the subcutaneous tissue. Persistent hyperemia. Detachment of the epidermis.
Degree III: destruction of the skin down to the muscle layer with penetration into the muscle. A bedsore looks like a wound. There may be liquid discharge.
Grade IV: all soft tissues affected. The presence of a cavity exposing underlying tissue (tendons, even bone).
Causes of bedsores
To date, it has been established that the main causes of pressure ulcers are:
- continuous pressure,
- displacement forces,
- friction and moisture.
The following also play a major role in the development of ulcers:
- limited motor activity of patients,
- insufficient nutrition and care for the sick (dirty, dry skin, crumbs and small objects in the bed, folds, seams, buttons on linen),
- urinary and fecal incontinence.
In addition, significant risk factors are such concomitant diseases and conditions as:
- diabetes,
- Parkinson's disease,
- allergic reaction to skin care products,
- sweating at elevated temperatures
- paraplegia and exhaustion.
Social risk factors include:
- being male (Spector W.D., 1994),
- age of patients over 70 years old,
- lack of service personnel.
How do bedsores occur?
When continuous pressure occurs, compression of the blood vessels occurs, resulting in insufficient blood flow to the tissues. In the case when displacement of soft tissues is added to the compression, tension occurs on the vessels, causing thrombosis and the risk of rupture of small capillaries, which are very necessary for the exchange of substances between blood and tissues, which also leads to ischemia of soft tissues and skin (Witkowsky J.A. and Parish L.C. (1982), as well as Allman).
The combined effect of shear forces and continuous pressure can lead to the development of pressure ulcers even at low external pressure. Friction also plays an important role as it causes the skin's protective outer stratum corneum to peel off.
Muscle fibers are more sensitive to the ischemic factor than the skin. Changes in response to pressure develop primarily in the muscle layer over the bony prominence. They subsequently spread towards the skin. Displacement forces play a decisive role in the formation of ulcers.
R.A. and Desforges J.F. (1989) conducted a number of experimental and clinical studies and scientifically proved the high risk of skin moisture and environment in the formation of pressure ulcers.
Prolonged exposure to continuous pressure leads to local tissue ischemia. As a result of special studies, it has been demonstrated that continuous pressure of 70 mm Hg. within 2 hours causes irreversible changes in tissues. At the same time, when the pressure stops every 5 minutes, minimal changes occur in the tissues without any consequences (Kosiak M., 1961).
Places of formation of bedsores.
Depending on the patient's position (on his back, on his side, sitting in a chair), the pressure points change.
Most often in the areas:
- auricle,
- thoracic spine (the most prominent part),
- sacrum,
- greater trochanter of the femur,
- protrusion of the fibula,
- ischial tuberosity,
- elbow,
- heels
Less commonly in the area: occiput, mastoid process, acromion process of the scapula, spine of the scapula, lateral condyle, toes.
In world practice, there are cases of localization of bedsores on the fingers, as well as on the head and ears. A bedsore on the skin can also arise from the pressure of a plaster cast during fractures or on the mucous membrane of the mouth - from the pressure of a denture.
Prevention of bedsores.
Principles of prevention:
- reducing compression, friction, or shear;
- proper nutrition and personal hygiene;
- reduction of skin irritants;
- skin care - keep your skin clean;
- decreased skin moisture;
- regularity and correctness of discharge (urine and feces).
Reducing compression
A soft but resilient mattress is required. A foam mattress is suitable for this, the thickness of which should be at least 15 cm. The bed should be flat without bumps or pits. You can purchase a special anti-bedsore mattress, but remember that it is not a panacea for bedsores; if other measures are not taken, the patient lying on it can still develop bedsores. Inspect your skin daily, especially in areas of bony prominences, as... This is where bedsores form. It is necessary to frequently change the position of the patient's body so that the skin experiences minimal friction and the soft tissue experiences minimal displacement. This must be done at least every 2-3 hours, including at night. Additional cushions are placed under the bone protrusions, for example, soft pillows made of feathers or foam rubber. Under motionless limbs, you can sew bags filled with round grains, for example, millet. A rubber circle is placed under the sacrum. The point of using a variety of bolsters and anti-bedsore mattresses is that they increase the area of contact between the body and the surface on which the patient lies, which means that the pressure on each part of the body is reduced, circulatory impairment is reduced and thus the risk of bedsores is reduced. Do not lift a patient alone if the patient cannot help you. Do not drag or pull out underwear from under the patient, especially when it is wet. Don't push the boat underneath it. For all this there are simple techniques, the main meaning of which is that the patient must first be lifted, and only then moved or placed something under him. Do not leave the patient in an uncomfortable position, and do not try to seat weak patients or give them a semi-sitting position, because their muscle activity is not enough to maintain this position, and they begin to slide. Provide such patients with a support (any device for support) in the legs.
Food and drink
Drinking and nutrition should be complete, taking into account restrictions, if any. Food must contain at least 20% protein. Choose products that contain many microelements - iron and zinc, as well as vitamin C. Use fermented milk products, herbs, vegetables, and fruits. For seriously ill patients, meat is a difficult food. Use chicken broth, fish, beans, grains and dairy products to meet your protein needs. Drink at least 1.5 liters, unless there are restrictions. Do not consume sugary and carbonated drinks, as well as freeze-dried foods, i.e. instant cooking from dry substances by dissolving in water.
Reduced skin irritation
Lay out old, washed, and therefore soft underwear; Make sure that there are no rough seams, buttons, or patches on the linen; Straighten the bed regularly and often so that there are no folds or small objects under the patient. Use low-allergenic, proven products for skin care, such as baby soap. Avoid substances that are bright in color or have a strong odor. Perineal toilet more often, because... particles of feces and urine are strong irritants. Under no circumstances should you limit the drinking capacity of a patient with urinary incontinence. with a lack of fluid, the concentration of urine increases, and, accordingly, the strength of irritation. Cut your and the patient's nails short: for yourself so as not to accidentally scratch the patient, and for the patient so that he does not scratch the skin, because. When lying or sitting for a long time, the compressed areas itch. Make sure that the patient is dressed and covered with a blanket according to the temperature conditions of the room. When the patient overheats, sweating increases and the risk of developing bedsores increases.
Skin care rules
The rules are quite simple: do not allow the skin to get dirty, excessively dry and wet, because such skin is least able to resist external influences, use plain water, soap, a washcloth made of cotton fabric or a natural sponge, nourishing and moisturizing creams, drying ointments, powder . Watch your skin carefully and it will become clear to you when to apply what. The general rule is this: wet skin needs to be dried, and dry skin needs to be moisturized. Do not use antibacterial soap because... along with harmful bacteria, beneficial microorganisms are also destroyed; after stopping the use of such soap, the skin becomes less able to resist even a minor infection (advertising tells the truth, but not the whole truth). Alcohol-containing products such as lotions and camphor alcohol should only be used for patients with oily skin. Do not rub the leather in pressure areas when washing. Use soft sponges and use them very delicately so as not to injure the upper layers of the skin. When drying the skin, do not wipe it, but blot it. Never massage reddened areas of the skin, but light regular massage around these areas is highly desirable. Be sure to give your skin air baths.
The condition of the skin is significantly affected by moisture, mainly urine and sweat. The main thing is the patient’s personal hygiene and change of linen. Do this often. For urinary incontinence, it is better to use pads or diapers, although for some patients it is enough to just give the bedpan more often. In the absence of funds for pads and diapers, try to use diapers made from linen (folded cotton underwear placed in the crotch or placed under the buttocks will limit the spread of urine; old washed underwear absorbs moisture well). For urinary incontinence in men, a special urine collection system (urinal bag) can be used. Increased sweating is observed in patients with fever. In order to reduce sweating, you must first treat the underlying disease. To wipe the patient, it is better to use not soap and water, but a weak solution of vinegar (1 tbsp. table vinegar for 1 glass of water).
Treatment of bedsores.
You should not rely on the help of ointments, powders and other drugs until you free the affected areas from compression so that blood can freely flow to the site of the formed bedsore.
Speaking about the treatment of bedsores, it is necessary, first of all, to say a few words about wounds in general. How does a wound appear and develop? First, a damaging force acts on the tissue (in the case of pressure ulcers, this damaging force is represented by compression), which causes malnutrition and then tissue necrosis. The damaging force is not constant. If its effect is weakened or stopped, blood circulation at the site of injury will be restored. This will lead to rejection of the resulting necrosis (bedsore) and gradual healing of the wound through granulation and epithelization. Treatment of bedsores, therefore, comes down to three principles:
- restore blood circulation at the site of injury as much as possible;
- promote the rejection of necrotic masses (the bedsore itself);
- promote rapid healing of the cleaned wound.
Restoration of blood circulation
To restore blood circulation, it is necessary to use all the principles of prevention in combination (see above).
Rejection of necrotic masses
To reject necrosis use:
- mechanical removal of necrotic masses by surgery;
- the use of drugs that accelerate spontaneous rejection: Iruksol ointment. As a good home remedy, you can use wet dressings with a cognac salt solution (30 g of table salt and 150 ml of cognac). To reject necrosis, the bandage must be applied under compress paper and changed as necessary. Before applying a new dressing, be sure to wash the wound to avoid increasing the salt concentration.
Treatment of a cleared wound
It is necessary to create moist conditions for keeping the wound, using, for example, alginates (in the form of wipes and powder for filling wounds), hydrocolloid dressings (Hydrocoll, Duoderm, Hydrosorb, etc.), which help clean and close the wound. These bandages are quite expensive. To heal a wound, you can use a wide variety of healing agents: ointments "Levosin", "Levomikol", "Actovegin", "Solcoseryl", sea buckthorn oil and many others. Often, bedsores are complicated by the addition of a secondary infection, and then it is necessary to use antiseptic and antibacterial agents, such as boric acid, white streptocide powder, 3% hydrogen peroxide solution, furacillin solution 1:5000, Levomikol, Levosin ointments. In severe cases, in weakened and elderly patients, the use of antibacterial drugs orally is indicated.
Large area and difficult to heal bedsores can sometimes be cured only surgically - tissue transplantation.
When treating bedsores, bandages must be used. Where possible, use a bandage to secure the dressings; in other cases, use adhesive tape. Not every patch is suitable for this. Bedsores need to be treated for a long time, which means that the plaster will have to be used for a long time. What problems might arise from this? The patch interferes with the normal functioning of the skin (breathing, secretion, etc.). When the patch is removed, the surface layer of skin cells comes off, causing long-term use the patch may cause additional wounds. To avoid such complications, use a paper-based patch - the skin underneath breathes well, and the glue fixes the bandage well, but does not tear off cells from the surface of the skin when removing the patch. When applying the patch, do not pull it too tightly to avoid the formation of small skin folds, and also take into account the fact that when the patient’s position changes, the soft tissues will shift and stretch, which can lead to the formation of unwanted skin folds.
The skin around the bedsore requires the most careful care. It must be washed with soap. There is no need to be afraid that soap suds will get into the wound - this will not worsen the condition of the bedsore. When washing, do not rub the skin, but only blot it. After washing, it is necessary to either dry the skin on its own, or you can use one of the following preparations: 1% solution of potassium permanganate, brilliant green, ointments containing zinc. The latter remedy is preferable to others, since when used, gauze bandages do not stick to the edges of the wound and, accordingly, do not injure the newly formed epithelium and granulations when the bandage is removed.
When applying bandages to deep bedsores, the wounds must be tamponed (closed) to the full depth with a bandage, but not tightly, but loosely.
The clinical picture is different at different stages of development of pressure ulcers:
Stage 1: persistent skin hyperemia that does not go away after the pressure stops; the skin is not damaged.
Stage 2: persistent skin hyperemia; epidermal detachment; superficial (shallow) violation of the integrity of the skin (necrosis) spreading to the subcutaneous tissue.
Stage 3: destruction (necrosis) of the skin down to the muscle layer with penetration into the muscle; There may be liquid discharge from the wound.
Stage 4: damage (necrosis) of all soft tissues; the presence of a cavity in which tendons and/or bone formations are visible.
Places of possible formation of bedsores:
In a sitting position In a supine position

Lying on your side

Rice. 8. Places of formation of bedsores
Risk factors
Three main factors have been identified that lead to the formation of bedsores: pressure, shear force and friction. There are other reasons that predispose to the development of bedsores against the background of these factors. They are classified as internal and external, reversible and irreversible factors.

Rice. 9. Areas of greatest pressure and placement of pillows and circles to prevent bedsores.
Assessing the risk of developing pressure ulcers
The key to effective pressure ulcer prevention is assessing the risk of developing pressure ulcers. Currently, several scales exist to quantify the risk of developing pressure ulcers. The most universal from the point of view of use in departments of health care facilities of various profiles is the Waterlow scale for assessing the risk of developing pressure ulcers. The map she proposed was supposed to help understand the factors influencing the occurrence of pressure ulcers, provide a methodology for assessing the risk of developing pressure ulcers, and develop adequate tactics for prevention and/or treatment.
Interpretation of parameters for patient assessment
1. Body build (the ratio of the patient’s body weight and height)
Excess weight increases pressure mainly on those areas of the body where the skin is closest to the bone tissue. Due to tissue compression, blood circulation deteriorates, which leads to disruption of tissue metabolism.
The ratio of the patient's body weight and height can be determined by the body mass index (weight in kg divided by height in meters squared).
2. Urinary incontinence
Moisture and uric acid can quickly lead to maceration of the skin, thereby reducing its strength threshold. Particular attention should be paid to material that comes into contact with the patient's skin. Fabrics that do not allow moisture to pass through (oilcloth) and are used as lining material create conditions for maceration of the skin. In addition, it is necessary to control the condition of the bed linen, eliminating the possibility of folds that create additional pressure on the surface of the patient’s body.
3. Skin type. Visual risk areas
Cigarette paper often occurs in elderly patients or in patients taking high doses of steroid drugs for a long time. The skin is brittle, which increases the risk of damage.
Dry skin. Very dry skin is susceptible to the formation of long-term non-healing cracks. This, in turn, increases the likelihood of infection and the development of bedsores. It is necessary to use unscented moisturizers, which should be gently applied to the skin, avoiding rubbing.
Swelling skin. A characteristic feature of this type is stretching of the skin. This leads to deterioration of blood circulation and innervation of the skin. Bedsores that form with this type of skin are difficult to heal, since the skin’s ability to regenerate is reduced.
Sticky skin. With this skin condition, it is advisable to use a double-sided permeable mattress cover that absorbs moisture well and at the same time prevents it from returning to the surface.
Change in skin color, as a rule, is a sign of developing bedsores. Compression and stretching of tissue in the area of maximum pressure leads to impaired blood circulation in areas of the skin located above the damaged area, to the death of skin cells and the formation of deep bedsores.
Blemishes or damaged skin- these are already bedsores. Bacterial flora penetrates the body, creating conditions for further tissue damage and the spread of infection throughout the body.